- Calls to this hotline are currently being directed to Within Health or Eating Disorder Solutions
- Representatives are standing by 24/7 to help answer your questions
- All calls are confidential and HIPAA compliant
- There is no obligation or cost to call
- Eating Disorder Hope does not receive any commissions or fees dependent upon which provider you select
- Additional treatment providers are located on our directory or samhsa.gov
Bone Health in Girls with Eating Disorders
Contributor: Amelia Mostovoy from Adolescent Neuroendocrine Unit Massachusetts General Hospital
Why Does Bone Density Matter for Bone Health in Girls?
Bones provide our body not only with structure and support but also protect our vital organs. A common misconception is that bone health and osteoporosis are concerns only for older women, when in actuality; adolescence is the most important time for optimizing bone health in girls.
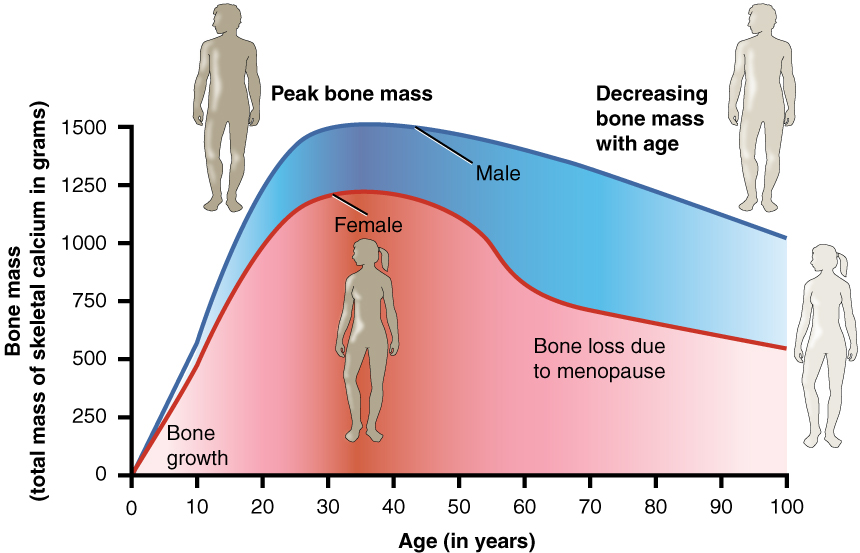
Bone mass increases rapidly during the teenage years, and we build 90% of our peak bone mass, all the bone we will ever have, by the time we are 18-20 years old. Our bones are at their strongest at peak bone mass. Also, the higher one’s peak bone mass, the lower risk there is for fracture in later life.
Adolescence is a critical window in time during which to optimize bone accrual and peak bone mass, and adolescence is thus the time where we can make or break bone health in girls for life. Armed with the knowledge that everyone loses bone as they age, and that having an eating disorder is a major risk factor for low bone density, it is important to take action to build bone mass while you still can.
Role of Genetics, Calcium, Vitamin D and Hormones
Click to Enlarge
An individual’s bone density is determined to a great extent by his/her genetic make-up. However, the remainder is largely under our control, with diet being a key component. Bones are our body’s warehouse, storing about 99% of all the calcium in the body.
Calcium is needed to keep muscles and nerves in working order. If the body is calcium deficient from lack of proper nutrition, blood will rob bones of calcium to maintain normal calcium levels in blood for vital functions, leading to weaker bones. Vitamin D is essential to absorb dietary calcium, and vitamin D deficiency thus leads to weaker bones and poorer bone health in girls.
The Benefits of Hormones
In addition, hormones such as estrogen and insulin-like growth factor-1 (IGF-1) play a key role in optimizing bone density during puberty. IGF-1 is essential for increasing bone formation, while estrogen prevents bone loss. Bones are constantly changing, with old bone being recycled and replaced with new bone.
Estrogen and IGF-1 also play a direct role in bone turnover with estrogen limiting bone loss while IGF-1 adds to bone mass.
Why Having an Eating Disorder Puts Bone Health in Girls at Risk
People affected by anorexia nervosa suffer from many nutritional and hormonal deficiencies and many experience low bone density. In fact, more than 50% of girls with anorexia nervosa show a significant bone loss in less than one year [1].
Dietary restriction leads to (i) low levels of estrogen and increased bone loss, and (ii) reduced IGF-1 secretion and thus reduced bone formation. This double whammy explains why girls suffering from anorexia nervosa, especially in their teenage years, are at risk for not attaining their full potential for peak bone mass.
Also, disease onset in adolescence (thus prior to attainment of peak bone mass), leads to worse bone outcomes compared to disease onset in adulthood, even when other factors are similar. Among girls 12 to 22 years old, those with anorexia nervosa have a 1.6 times greater risk of fracture than those without anorexia nervosa [2].

What Can You Do?
An important question is: what can you do to help your bones? The best strategy is to regain and maintain a healthy weight. However, sometimes weight restoration alone cannot make up for lost time.
If you think you are at risk for low bone density, having a bone density test is a good starting point. Through our work in the Neuroendocrine Unit at Massachusetts General Hospital, we have shown that replacing estrogen using a patch, rather than as a pill, helps prevent further bone loss in girls with anorexia nervosa [3].
Clinical Trials for Improving Bone Health in Girls
However, bone density does not normalize, likely because other hormone deficiencies, such as of IGF-1, persist. In our current clinical trial, we are assessing whether adding IGF-1 to estrogen replacement is effective in further increasing and potentially normalizing bone density in girls and young women with anorexia nervosa.
Bone density scans are available at Massachusetts General Hospital as well as compensation if you participate in this research trial. If you are interested in participating, please complete this survey. For more information about our research, please visit our website.
References:
1. Misra M, Aggarwal A, Miller KK, Almazan C, Worley M, Soyka LA, Herzog DB, Klibanski A: Effects of anorexia nervosa on clinical, hematologic, biochemical, and bone density parameters in community-dwelling adolescent girls. Pediatrics 2004, 114:1574-1583.
2. Faje AT, Fazeli PK, Miller KK, Katzman DK, Ebrahimi S, Lee H, Mendes N, Snelgrove D, Meenaghan E, Misra M, Klibanski A: Fracture risk and areal bone mineral density in adolescent females with anorexia nervosa. The International journal of eating disorders 2014, 47:458-466.
3. Misra M, Katzman D, Miller KK, Mendes N, Snelgrove D, Russell M, Goldstein MA, Ebrahimi S, Clauss L, Weigel T, et al: Physiologic estrogen replacement increases bone density in adolescent girls with anorexia nervosa. Journal of bone and mineral research : the official journal of the American Society for Bone and Mineral Research 2011, 26:2430-2438.
The opinions and views of our guest contributors are shared to provide a broad perspective on eating disorders. These are not necessarily the views of Eating Disorder Hope, but an effort to offer a discussion of various issues by different concerned individuals.
We at Eating Disorder Hope understand that eating disorders result from a combination of environmental and genetic factors. If you or a loved one are suffering from an eating disorder, please know that there is hope for you, and seek immediate professional help.
Published August 7, 2014, on EatingDisorderHope.com
Reviewed & Updated on June 6, 2019, by Jacquelyn Ekern MS, LPC
